
Welcome to our in-depth exploration of ATI real life postpartum hemorrhage, a topic that demands attention due to its profound impact on maternal health. This guide will immerse you in the complexities of PPH, equipping you with the knowledge and strategies to navigate this critical obstetric emergency.
Delving into the intricacies of PPH, we will dissect its definition, classification, risk factors, clinical presentation, and diagnosis. We will meticulously examine the management strategies, encompassing both pharmacological and non-pharmacological interventions. A comparative table will shed light on the nuances of different uterotonic agents employed in PPH management.
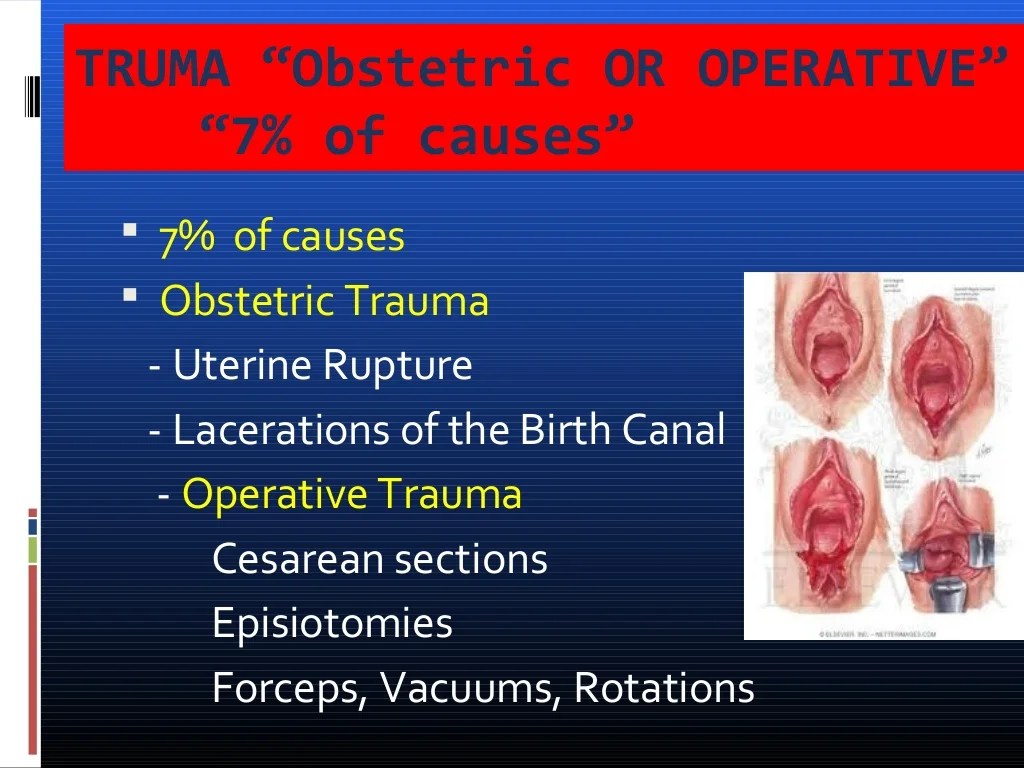
Postpartum Hemorrhage (PPH) Definition and Classification
Postpartum hemorrhage (PPH) is defined as excessive bleeding from the genital tract following childbirth. It is a life-threatening obstetric emergency that requires prompt recognition and management.
PPH is classified based on the time of onset:
Primary PPH
Primary PPH is bleeding that occurs within 24 hours of delivery. It is the most common type of PPH, accounting for approximately 80% of cases.
Secondary PPH
Secondary PPH is bleeding that occurs between 24 hours and 12 weeks after delivery. It is less common than primary PPH, accounting for approximately 20% of cases.
Risk Factors for PPH
Postpartum hemorrhage (PPH) is a significant complication that can occur during or after childbirth. Various factors can increase the risk of developing PPH, and understanding these risk factors is crucial for healthcare providers to identify and manage patients at risk.
Risk factors for PPH can be classified into two categories: modifiable and non-modifiable.
Modifiable Risk Factors
- Uterine atony:Failure of the uterus to contract adequately after delivery, leading to continued bleeding.
- Placental abnormalities:Retained placenta or placental fragments, which can prevent proper uterine contraction and cause bleeding.
- Excessive blood loss during labor:This can deplete the mother’s blood volume and increase the risk of PPH.
- Prolonged labor:Extended labor can exhaust the uterus and make it less effective in contracting.
- Induction or augmentation of labor:These interventions can increase uterine contractions, potentially leading to uterine overstimulation and PPH.
- Multiple pregnancies:Women with multiple pregnancies have an increased risk of uterine overdistention and PPH.
- Obesity:Obesity can contribute to uterine atony and make it difficult to control bleeding.
- Smoking:Smoking during pregnancy can impair uterine contractility.
- Preeclampsia:This condition can lead to placental abruption or other complications that increase the risk of PPH.
Non-Modifiable Risk Factors
- Advanced maternal age:Women over the age of 35 have an increased risk of PPH.
- History of PPH:Women who have experienced PPH in previous pregnancies are at higher risk for recurrence.
- Uterine anomalies:Certain uterine abnormalities, such as a bicornuate uterus, can increase the risk of PPH.
- Coagulopathies:Disorders that affect blood clotting, such as hemophilia or thrombocytopenia, can increase the risk of excessive bleeding.
Clinical Presentation and Diagnosis of PPH
Postpartum hemorrhage (PPH) is a life-threatening obstetric emergency that requires prompt recognition and management. Early identification and diagnosis are crucial for successful treatment and prevention of maternal morbidity and mortality.
Clinical Signs and Symptoms of PPH
- Vaginal bleeding:Excessive or persistent vaginal bleeding that exceeds 500 ml after vaginal delivery or 1000 ml after cesarean delivery.
- Hemodynamic instability:Signs of shock, such as tachycardia, hypotension, tachypnea, and oliguria.
- Pallor:Pale skin, mucous membranes, and nail beds.
- Uterine atony:A soft, boggy uterus that does not contract effectively.
- Clots:Passage of large or numerous blood clots.
- Fetal distress:Signs of fetal compromise, such as bradycardia or decreased fetal movement.
Methods Used to Diagnose PPH
- Clinical assessment:Physical examination and history, including assessment of vaginal bleeding, hemodynamic status, and uterine tone.
- Hemoglobin and hematocrit levels:Serial blood tests to monitor hemoglobin and hematocrit levels, which can indicate the severity of blood loss.
- Ultrasound:Transvaginal or abdominal ultrasound can visualize the uterus and identify potential causes of PPH, such as retained placenta or uterine rupture.
- Laparotomy:In severe cases, laparotomy may be necessary to explore the abdomen and identify the source of bleeding.
Management of PPH
Postpartum hemorrhage (PPH) is a life-threatening obstetric emergency that requires prompt and effective management to prevent maternal morbidity and mortality. The management of PPH involves a multidisciplinary approach, including immediate resuscitation measures, pharmacological interventions, and surgical interventions if necessary.
Immediate Steps
The immediate steps taken to manage PPH include:
- Call for help:Activate the obstetric emergency response team and request assistance from other healthcare providers.
- Secure the airway:Ensure the patient has a patent airway and administer oxygen as needed.
- Establish intravenous access:Insert two large-bore intravenous catheters to administer fluids and medications.
- Measure blood loss:Estimate the amount of blood loss using a graduated bedpan or weighing the pads.
- Replace blood loss:Transfuse blood products as indicated based on the patient’s vital signs and hemoglobin levels.
Pharmacological Interventions
Pharmacological interventions used to control bleeding in PPH include:
- Uterotonic agents:These medications stimulate uterine contractions to reduce bleeding. Examples include oxytocin, carboprost, and misoprostol.
- Vasopressors:These medications increase blood pressure and reduce bleeding. Examples include vasopressin and norepinephrine.
- Antifibrinolytic agents:These medications prevent the breakdown of blood clots and reduce bleeding. Examples include tranexamic acid and epsilon-aminocaproic acid.
Non-Pharmacological Interventions
Non-pharmacological interventions used to control bleeding in PPH include:
- Uterine massage:Manually massaging the uterus helps to stimulate contractions and reduce bleeding.
- Bimanual compression:Applying pressure to the uterus with one hand vaginally and the other hand abdominally helps to control bleeding.
- Intrauterine balloon tamponade:A balloon is inserted into the uterus and inflated to compress the uterine walls and stop bleeding.
- Surgical interventions:Surgical interventions may be necessary if conservative measures fail to control bleeding. These interventions include uterine artery embolization, hysterectomy, and uterine repair.
Table of Uterotonic Agents
The following table compares the different uterotonic agents used in PPH management:
| Agent | Mechanism of Action | Dose | Route of Administration | Side Effects |
|---|---|---|---|---|
| Oxytocin | Stimulates uterine contractions | 10-40 units in 1000 mL of IV fluid | Intravenous infusion | Hypotension, nausea, vomiting |
| Carboprost | Stimulates uterine contractions and vasoconstriction | 250-500 mcg intramuscularly | Intramuscular injection | Nausea, vomiting, diarrhea, bronchospasm |
| Misoprostol | Stimulates uterine contractions and reduces prostaglandin production | 600-1000 mcg sublingually or vaginally | Sublingual or vaginal administration | Nausea, vomiting, diarrhea, uterine rupture |
Complications of PPH
Postpartum hemorrhage (PPH) can lead to a range of short-term and long-term complications, significantly impacting maternal health and well-being.
Short-term complicationsof PPH include:
- Hypovolemic shock: Severe blood loss can lead to a drop in blood volume, resulting in shock, organ damage, and even death.
- Disseminated intravascular coagulation (DIC): A condition where the blood clotting system becomes overactive, leading to widespread clotting and bleeding.
- Acute kidney injury: Severe blood loss can damage the kidneys, leading to acute kidney failure.
- Uterine atony: The uterus fails to contract effectively, leading to continued bleeding.
Long-term complicationsof PPH include:
- Iron deficiency anemia: Severe blood loss can lead to a deficiency of iron, which is essential for red blood cell production.
- Pelvic organ prolapse: Damage to the pelvic floor muscles during PPH can lead to prolapse of the uterus, bladder, or rectum.
- Infertility: Severe PPH can damage the reproductive organs, leading to infertility.
- Postpartum depression: The physical and emotional trauma of PPH can increase the risk of postpartum depression.
PPH is a serious condition that can have significant consequences for maternal health and well-being. Early recognition and prompt treatment are essential to prevent these complications.
Prevention of PPH
Prevention of postpartum hemorrhage (PPH) is crucial to ensure maternal well-being and reduce associated risks. Evidence-based strategies implemented during antenatal care, intrapartum management, and postpartum care play a vital role in minimizing the incidence and severity of PPH.
During antenatal care, early identification of risk factors, such as previous PPH, multiple gestation, and uterine abnormalities, allows for targeted interventions and monitoring.
Intrapartum Management
Effective intrapartum management strategies include:
- Active management of the third stage of labor using uterotonics, such as oxytocin or misoprostol, to promote uterine contractions and reduce blood loss.
- Controlled cord traction to avoid uterine inversion.
- Early recognition and management of risk factors, such as prolonged labor, shoulder dystocia, and uterine atony.
- Judicious use of episiotomy to prevent perineal lacerations that may contribute to PPH.
Postpartum Care
Postpartum care plays a critical role in PPH prevention and early detection:
- Frequent monitoring of vital signs, uterine tone, and vaginal bleeding for early identification of PPH.
- Uterine massage to promote uterine contractions and reduce bleeding.
- Encouraging early ambulation and breastfeeding to stimulate uterine contractions.
- Patient education on PPH risk factors, signs, and symptoms to facilitate self-monitoring and timely reporting.
Nursing Management of PPH
Nurses play a crucial role in the management of postpartum hemorrhage (PPH), providing comprehensive care to ensure the well-being of both the mother and newborn. Their responsibilities encompass assessment, monitoring, and implementation of interventions aimed at preventing and managing PPH effectively.
Assessment
Upon recognition of signs and symptoms suggestive of PPH, nurses promptly assess the patient’s condition to determine the severity and extent of bleeding. This includes monitoring vital signs, assessing vaginal bleeding, checking for uterine tone and size, and evaluating the patient’s overall appearance and behavior.
Monitoring
Continuous monitoring is essential to track the patient’s response to treatment and detect any changes in her condition. Nurses monitor vital signs, blood loss, uterine involution, and the patient’s response to medications and interventions. Regular assessments allow for timely adjustments to the treatment plan as needed.
Interventions
Nursing interventions for PPH are multifaceted and tailored to the patient’s individual needs. These may include:
- Administering medications to promote uterine contraction and reduce bleeding
- Providing uterine massage to stimulate uterine tone and reduce bleeding
- Applying ice packs to the perineum to reduce swelling and promote vasoconstriction
- Inserting a Foley catheter into the bladder to apply pressure on the uterus
- Preparing the patient for surgery if conservative measures fail to control bleeding
Education and Counseling for PPH
Patient education and counseling play a crucial role in reducing the incidence and severity of postpartum hemorrhage (PPH). By providing comprehensive information about risk factors, signs, symptoms, and management strategies, healthcare providers can empower patients to recognize and respond to PPH promptly.
Effective education and counseling should include the following:
Risk Factor Awareness
- Discuss the various risk factors for PPH, such as multiple pregnancies, previous uterine surgery, prolonged labor, and retained placenta.
- Emphasize the importance of identifying and managing these risk factors during pregnancy and labor.
Signs and Symptoms Recognition
- Explain the common signs and symptoms of PPH, including heavy vaginal bleeding, hypotension, tachycardia, and pallor.
- Instruct patients to seek immediate medical attention if they experience any of these symptoms after delivery.
Management Strategies
- Review the different treatment options for PPH, such as uterine massage, oxytocin administration, and surgical intervention.
- Provide guidance on the importance of adhering to prescribed medications and follow-up appointments.
Prevention Measures
- Discuss the importance of prenatal care, including regular checkups and monitoring for risk factors.
- Explain the benefits of labor management techniques that can reduce the risk of PPH, such as controlled cord traction and avoiding excessive fundal pressure.
By providing comprehensive education and counseling, healthcare providers can equip patients with the knowledge and skills necessary to prevent, recognize, and manage PPH, ultimately improving maternal outcomes and reducing the risk of complications.
Case Study or Real-Life Scenario: Ati Real Life Postpartum Hemorrhage
A 25-year-old primigravida presented with a sudden onset of heavy vaginal bleeding, dizziness, and hypotension 2 hours after vaginal delivery. She had a history of gestational hypertension and was induced at 39 weeks gestation for severe preeclampsia. The labor was uncomplicated, and the baby was born weighing 3,200 grams with Apgar scores of 8 and 9 at 1 and 5 minutes, respectively.
The placenta was delivered intact, and there were no apparent lacerations or uterine atony.
Upon examination, the patient was pale, diaphoretic, and tachycardic. Her hemoglobin level had dropped from 12 g/dL to 8 g/dL. A bimanual examination revealed a soft and boggy uterus, and there were no signs of retained placental fragments. The bleeding continued despite conservative management with intravenous fluids, uterotonics, and uterine massage.
Management
Given the patient’s persistent bleeding and hemodynamic instability, a decision was made to proceed with surgical intervention. An exploratory laparotomy was performed, and a uterine atony was identified as the source of the hemorrhage. The uterus was sutured, and the bleeding was controlled.
The patient received a blood transfusion and was transferred to the intensive care unit for monitoring. She made a full recovery and was discharged from the hospital 3 days later.
Outcomes, Ati real life postpartum hemorrhage
The patient experienced no long-term complications from the postpartum hemorrhage. She had a normal subsequent pregnancy and delivery.
Quick FAQs
What are the common risk factors for ATI real life postpartum hemorrhage?
Modifiable risk factors include prolonged labor, uterine atony, retained placenta, and episiotomy. Non-modifiable risk factors include multiple gestation, previous PPH, and uterine anomalies.
How is ATI real life postpartum hemorrhage diagnosed?
Diagnosis involves assessing vital signs, estimating blood loss, and performing a physical examination to identify the source of bleeding.
What are the immediate steps taken to manage ATI real life postpartum hemorrhage?
Immediate steps include administering oxygen, establishing intravenous access, and initiating fluid resuscitation. Uterine massage and pharmacological interventions may also be employed.
